
The August issue of Health Affairs, a variety issue, includes a collection of articles that show the extent of health disparities in the United States and describe approaches designed to address them. There are also articles covering hospital financing, Medicare, and other topics.
Documenting active life expectancy disparities: black and white differences remain
Research previously published, in Health Affairs and elsewhere, has described racial differences in life expectancies. However, very few studies have focused on long-term trends in active life expectancy by race.
Vicki Freedman of the University of Michigan and Brenda Spillman of the Urban Institute looked at data from the 1982 and 2004 National Long Term Care Surveys and the 2011 National Health and Aging Trends Study to compare black and white racial differences in postponing disability. According to the authors, while life expectancy has risen for both groups, whites can expect to live disability-free for three-quarters of the remaining years of their lives, compared to two-thirds of remaining years for blacks. The authors note that the black-white gaps persisted largely because of the lack of progress for older black women in gaining years of active life. Their findings suggest that research pinpointing which measures reduce disparities in dependence is needed to address pressures on the long-term care delivery system as a result of population aging.
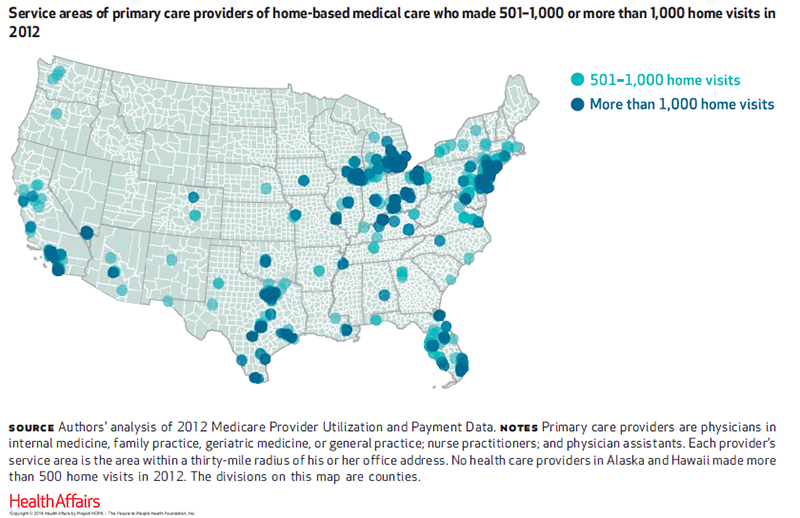
DATAWATCH: Geographic concentration of US home-based medical care providers
As many as four million US residents need home-based medical care, and there is a shortage of willing providers. Nengliang (Aaron) Yao of the University of Virginia School of Medicine and coauthors used 2012–13 Medicare fee-for-service data and found that 9 percent of the 5,000 primary care providers performed 44 percent of the 1.7 million home visits that year (See map below). The authors also determined that the majority of Americans live more than 30 miles from a home-based medical care provider.
The data, the authors note, suggest a mismatch between the medical needs of homebound older adults and the ability of the medical system to provide care for them where they need to be served. This is one of the first descriptions of the provision and use of US home-based medical care and sets a baseline for future evaluation of workforce and geographic variations in its composition and use.
DATAWATCH: Language services in US hospitals vary by location and ownership
According to the Census Bureau, 24 million US residents have limited English proficiency and, as a result, could encounter difficulties when communicating with health care providers. Melody Schiaffino of the San Diego State University and coauthors compared the availability of language services and the need for them across 4,514 general US hospitals using 2013 data from the American Hospital Association’s Annual Survey of Hospitals.
The study found that 68.8 percent of them offered language services nationwide, with a large gap between the services offered by ownership status and location. According to the authors, the majority of private not-for-profit hospitals offered language services, as opposed to fewer than 20 percent of private for-profit and government hospitals. Since federally funded health care institutions, including hospitals, are required to provide language services to patients with limited English proficiency, the authors found this pattern concerning. They recommend that hospitals failing to provide language services need to be made aware of patients’ right to receive care in a language they understand.
Sight-threatening diseases go undiagnosed among poor children
Early detection and treatment of common childhood eye diseases can lead to better long-term visual outcomes. Joshua Stein of the University of Michigan and coauthors analyzed health care claims data for nearly 900,000 children with commercial health insurance to determine whether household net worth affected rates of visits to ophthalmologists and optometrists and diagnosis rates of strabismus (misaligned eyes) and amblyopia (lazy eye).
The authors found that despite the fact that all of the children were covered by the same health insurance plan, children in more affluent families tended to use more eye care services than did less affluent children. Their data also revealed that rates of strabismus and amblyopia diagnoses were higher in children of more affluent families, suggesting that these sight-threatening conditions might be going undetected in children from less affluent families. The authors describe ways to improve screening and detection of common ocular diseases to reduce disparities in care among less affluent children.
Another disparity-related study in the August issue:
And the August Narrative Matters essay, by a former Health and Human Services Secretary:
Hospital Medicare rates: Medicare Advantage versus fee-for-service
Most Medicare analyses are based exclusively on fee-for-service claims, overlooking the fastest-growing part of that program: Medicare Advantage, which now enrolls almost one-third of Medicare beneficiaries. Laurence Baker of Stanford University and coauthors examined data from 2009 and 2012 from the Health Care Cost Institute as well as Medicare data to determine hospital payment rates.
According to the authors, Medicare Advantage plans pay hospitals about 8 percent less than fee-for-service Medicare, with about one-third of that difference because of the Medicare Advantage plans’ narrower hospital networks. These findings suggest that the government’s ongoing efforts to adjust payments to Medicare Advantage, based on the Affordable Care Act, should consider the Medicare Advantage market environment more broadly, instead of just the level of fee-for-service Medicare spending.
ACA blocked formation and expansion of physician-owned hospitals
The Affordable Care Act (ACA) has imposed new restrictions, which took effect in 2010, on the formation and expansion of physician-owned hospitals. To determine whether the ACA motivated these hospitals to take certain preemptive actions and modify their operating practices to maintain or increase their profitability under these new restrictions, Elizabeth Plummer and William Wempe of Texas Christian University examined 106 physician-owned hospitals in Texas, a group comprising approximately 20 percent of hospitals in that state, before and after the restrictions were implemented. They found significant pre-ACA increases in the establishment of physician-owned hospitals.
According to the study, once the ACA provisions took effect, hospitals improved the use of their assets to generate increased amounts of services, revenue, and profits. However, the authors did not find evidence that these hospitals had stopped accepting Medicare patients to avoid the new restrictions. The study reports that thirteen physician-owned hospitals were established between 2011 and 2015 that adopted a policy of not accepting Medicare; all of them have now been sold or are part of bankruptcy filings. The authors conclude that the ACA has effectively eliminated the formation of new physician-owned hospitals.
Also of interest:
Latin American & Caribbean countries see gaps in primary care, health system performance
To examine the critical role of primary care in promoting overall health system performance in Latin American countries, James Macinko of the University of California, Los Angeles, and coauthors analyzed survey data from Brazil, Colombia, El Salvador, Jamaica, Mexico, and Panama for the year 2013. The authors found significant weaknesses in primary care, with more than half of respondents lacking a regular doctor.
According to the study, there were high rates of skipping needed care and accessing care on weekends. High emergency usage was also noted, along with an association between reporting a great number of primary care problems and the probability of using the emergency department for a condition treatable in primary care. Respondents’ reports of primary care experiences were strongly associated with assessments of how their health systems function, protect them from financial hardship, and deliver high-quality and appropriate care. The authors caution that urgent attention is needed as the population in these countries continues to age at an unprecedented rate.
Also of global interest in the August issue: